
Degenerative rotator cuff tears get more common as we age. Just as important, many of these tears show up on imaging in people who have little or no shoulder pain. That means an MRI finding does not automatically explain your symptoms, and it does not automatically mean you need surgery. For many adults, the best first step is a good exam and a progressive rehab plan.
Key takeaways
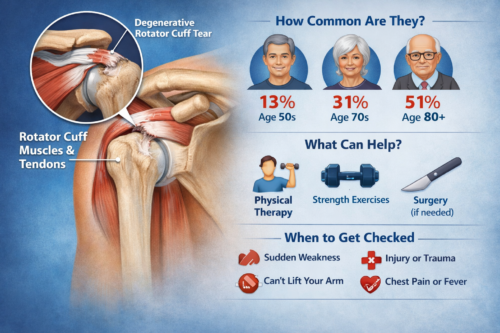
- Degenerative rotator cuff tears are age-related tendon tears that often happen gradually, not from one big injury.
- In symptom-free adults, full-thickness tears have been found in about 13% of people in their 50s, 20% in their 60s, 31% in their 70s, and 51% over age 80.
- In one population study, rotator cuff tears were present in 22.1% of adults overall, and asymptomatic tears were about twice as common as symptomatic tears.
- Physical therapy helps many people improve pain and function, though some tears can enlarge over time and some people do benefit from surgical consultation.
What is a degenerative rotator cuff tear?
The rotator cuff is a group of four muscles and tendons that help keep your shoulder stable and help you lift and rotate your arm. A degenerative tear means the tendon has changed over time from age, repeated loading, and tissue wear. That is different from an acute traumatic tear, which happens after a clear injury like a fall or sudden heavy lift. Rotator cuff problems often cause pain, weakness, and reduced motion, but not every tear is painful.
How common are degenerative rotator cuff tears as you age?
This is where the topic gets interesting.
A classic imaging study of adults with no shoulder symptoms found full-thickness tears in 13% of people ages 50 to 59, 20% ages 60 to 69, 31% ages 70 to 79, and 51% of people older than 80.
A larger systematic review that pooled data from 6,112 shoulders found that any rotator cuff abnormality increased from 9.7% in people age 20 and younger to 62% in people age 80 and older. The authors noted that these abnormalities were common even in people without symptoms.
Population-based data tell a similar story. In one study, rotator cuff tears were present in 22.1% of the general population, and asymptomatic tears were about twice as common as symptomatic tears. Another general-population study found full-thickness tears in 20.7% of 1,366 shoulders, with age as a major risk factor.
Why this matters
If shoulder pain starts and an MRI shows a tear, it is tempting to assume, “That must be the problem.” Sometimes it is. Sometimes it is only part of the picture.
Because degenerative rotator cuff tears are so common with age, the real question is not only “Is there a tear?” but also “Does it match your symptoms, exam findings, strength loss, and function?” That is one reason a careful clinical exam matters so much. Imaging can help, but it works best as an adjunct to the exam, not as the whole story.
What helps?
For many adults with gradual-onset shoulder pain, the first step is usually individualized conservative care.
The current AAOS guideline says both physical therapy and surgery can improve outcomes for symptomatic small-to-medium full-thickness tears. The same guideline also says patient-reported outcomes improve with physical therapy, even though some tears may enlarge over 5 to 10 years with non-operative care.
The newer rotator cuff tendinopathy guideline supported by APTA and published in JOSPT recommends an active rehabilitation exercise program, which may include shoulder mobility and resistance exercise. In plain language: movement and strength work matter. Rehab is usually more than rest, stretches, and waiting. The right plan allows you to build all your strength back and get all your flexibility back.
A good PT plan often includes:
- calming down painful movements without complete shutdown
- restoring shoulder range of motion
- building rotator cuff and shoulder-blade strength
- improving tolerance for reaching, lifting, work, and exercise
- progressing back to the activities that matter to you
This is where a program like Orthopedic & Sports Physical Therapy can be helpful, especially when it progresses into true loading and rebuilding through Strength Training Physical Therapy instead of stopping at band exercises forever.
Do you need imaging right away?
Not always.
Guidelines note that imaging is useful as an adjunct to the exam for identifying tears, but it is generally most helpful when there has been trauma, when there is concern for a significant structural lesion like a full-thickness tear, or when the result would change treatment decisions.
That means an MRI can be very useful in the right situation. It also means many people do not need immediate imaging on day one of shoulder pain.
When might surgery be worth discussing?
Surgery can be appropriate in some cases, especially when there is a confirmed full-thickness tear plus significant pain, major weakness, or meaningful loss of function. Early orthopedic referral is also more important after trauma, in younger or high-demand patients, and in some larger tears.
At the same time, it is important to consider that non-operative care can help symptoms even when the tendon does not “heal back together” on imaging. The tradeoff is that some tears can enlarge over time, which is why follow-up matters if weakness or function keeps slipping.
Try-this-today checklist
These are simple starting ideas, not a diagnosis:
- Sleep with the sore arm supported on a pillow.
- Temporarily cut back on repeated painful overhead work.
- Keep the shoulder moving in a comfortable range instead of completely resting it.
- Start guided strengthening once symptoms calm enough to tolerate it.
- Get assessed if pain is lingering, night pain is growing, or the arm feels weak.
Some people also do well with hands-on treatment as an add-on, not a replacement, for exercise. That can be a reasonable role for Manual / Massage Physical Therapy if stiffness is making it hard to start moving.
What to avoid
- assuming every MRI tear needs surgery
- stopping all shoulder use for weeks
- pushing through sharp pain just to “strengthen it”
- waiting too long if there was a sudden injury and new weakness
- basing treatment only on imaging instead of symptoms and function
When to seek urgent care
Seek urgent medical care if:
- you have immediate weakness after an injury
- you suddenly cannot move your arm
- the shoulder looks deformed or is badly swollen
- you feel feverish or unwell with shoulder pain
- shoulder pain comes with chest pressure, sweating, or trouble breathing
When to see a PT
See a PT when shoulder pain is not settling, when sleep is getting disrupted, when lifting or reaching feels weaker, or when you are no longer trusting the arm for daily tasks, work, or exercise. The earlier goal is often not “fix the image.” It is to improve pain, strength, movement, and confidence while helping you decide whether further imaging or referral is actually needed.
FAQ
If my MRI shows a tear, do I need surgery?
No. Many tears are age-related and painless, and both PT and surgery can improve outcomes in many small-to-medium full-thickness tears.
Can a degenerative rotator cuff tear heal on its own?
Symptoms and function can improve a lot with rehab, but the tendon itself may not fully restore on imaging. Some tears also enlarge over time, which is why follow-up matters.
Is exercise safe if I have a tear?
Usually, yes, when it is matched to your irritability, strength, and function. Current guidelines support active rehab, including exercise, as a core part of care.
When is imaging most useful?
Imaging is most useful when there was trauma, when a significant tear is suspected, when weakness is notable, or when the result will change next-step decisions.
Why Quincy Physical Therapy
At Quincy Physical Therapy, shoulder care is built around evidence-based progression: calm symptoms, restore motion, rebuild strength, and get back to real-life lifting and reaching. Even though the clinic is spine-focused, the same approach applies here: thoughtful loading, clear education, and strength programming that helps you move better for the long term.
If shoulder pain or weakness is hanging around, schedule a visit and get a plan that fits your shoulder, your goals, and your timeline.
References
- Tempelhof S, Rupp S, Seil R. Age-related prevalence of rotator cuff tears in asymptomatic shoulders. J Shoulder Elbow Surg. 1999.
- Teunis T, Lubberts B, Reilly BT, Ring D. A systematic review and pooled analysis of the prevalence of rotator cuff disease with increasing age. J Shoulder Elbow Surg. 2014.
- Minagawa H, Yamamoto N, Abe H, et al. Prevalence of symptomatic and asymptomatic rotator cuff tears in the general population: From mass-screening in one village. J Orthop. 2013.
- American Academy of Orthopaedic Surgeons. Management of Rotator Cuff Injuries: Clinical Practice Guideline. 2025.
- Desmeules F, Roy J-S, Lafrance S, et al. Rotator Cuff Tendinopathy Diagnosis, Non-surgical Medical Care and Rehabilitation: A Clinical Practice Guideline. J Orthop Sports Phys Ther. 2025.
- Grusky AZ, Giri A, O’Hanlon D, Jain NB. The Relationship of Aging and Smoking With Rotator Cuff Disease: A Systematic Review and Meta-analysis. Am J Phys Med Rehabil. 2022.