
Cervical Radiculopathy: Symptoms, Shoulder Blade Pain, and What Usually Helps
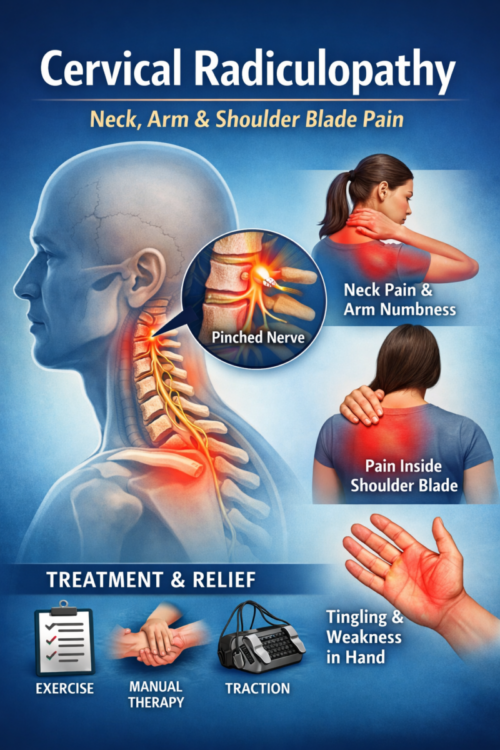
If you’ve ever felt neck pain that travels into your shoulder, inside the shoulder blade, arm, or hand—sometimes with tingling or numbness—you may be dealing with cervical radiculopathy. That’s the medical term for irritation or compression of a nerve root in your neck.
The good news: many cases improve with time and the right plan—often without injections or surgery. A physical therapist can help you calm symptoms down and rebuild strength and confidence with movement.
Key takeaways
-
Cervical radiculopathy can cause neck pain plus arm symptoms (pins/needles, numbness, or weakness).
-
Pain may also show up between the shoulder blades or “inside” one shoulder blade.
-
Helpful care often includes specific exercises, activity changes, and manual therapy; some people benefit from traction.
-
Get checked quickly if you notice progressive weakness, major balance issues, or other red flags (listed below).
What is cervical radiculopathy?
Your neck (cervical spine) has nerves that exit between the bones and travel to your shoulder, arm, and hand. Cervical radiculopathy happens when one of those nerve roots gets irritated—commonly from age-related changes, a disc bulge, or inflammation.
Plain-language definition: it’s a “pinched or irritated nerve” in the neck that can create symptoms anywhere along that nerve’s pathway.
Common causes
Cervical radiculopathy is often related to:
-
Disc-related irritation (a disc bulge/herniation)
-
Arthritis/degenerative changes that narrow the nerve opening (foraminal stenosis)
-
Inflammation around the nerve root
-
Less commonly: trauma, or other medical causes that need medical work-up
Signs and symptoms (including inside-the-shoulder-blade pain)
Symptoms vary by which nerve root is involved, but common patterns include:
-
Neck pain and stiffness
-
Pain that spreads into the shoulder, arm, or hand
-
Pain felt “inside” or along the border of the shoulder blade (interscapular pain)
-
Tingling/pins-and-needles or numbness in the arm/hand
-
Weakness (grip, triceps, biceps, shoulder)
-
Symptoms that change with neck position (often worse looking up/turning toward the painful side)
-
Sometimes: symptoms eased by resting the hand on the head (not always)
Why the shoulder blade can hurt
Even though the nerve irritation starts in the neck, pain can be referred to nearby areas—especially the shoulder blade region—because of how nerves and muscles share signaling pathways. It’s also common for the upper back/shoulder blade muscles to tighten up protectively when the neck is irritated.
What usually helps
A good plan aims to do two things:
-
Reduce nerve irritation and calm pain
-
Restore motion and strength so symptoms don’t keep coming back
Here are common components that PTs use (tailored to you):
1) Symptom-calming strategies (first 1–2 weeks for many people)
-
Finding positions that reduce symptoms (often neutral neck posture)
-
Short “movement snacks” during the day (gentle neck and upper back motion)
-
Modifying aggravating activities temporarily (more below)
-
Heat or ice if they help you tolerate movement (comfort measures)
Clinical guidelines support matching treatment to symptom irritability and using education + activity advice early.
2) Targeted exercises
A PT will choose exercises based on your pattern, such as:
-
Cervical retraction (chin tuck) variations to improve neck mechanics
-
Range-of-motion work that doesn’t spike arm symptoms
-
Scapular (shoulder blade) strength and endurance (mid/lower trap, serratus) through Strength Training and Performance programs
-
Deep neck flexor endurance work (front-of-neck support muscles)
-
Nerve mobility (“nerve glide”) exercises only if appropriate (these should feel gentle—not like a hard stretch)
Exercise-based care is strongly represented in neck pain guidance, including subgroups with radiating symptoms.
3) Manual therapy (when appropriate)
Hands-on treatment may include gentle mobilization of the neck and upper back, and soft-tissue work around the shoulder girdle to help you move more comfortably—especially if your shoulder blade area is tight and sore. Evidence suggests manual therapy can help pain and disability for cervical radiculopathy, usually as part of a broader plan.
4) Traction (for some people)
Mechanical traction (in-clinic) may help certain patients, especially when combined with exercise. It’s not right for everyone, and the decision should be based on your exam findings and tolerance.
Try-this-today checklist (safe starting points)
These are general options. Stop if symptoms sharply worsen down the arm/hand or if you feel increasing numbness/weakness.
-
Posture reset (30–60 seconds): Sit tall, relax shoulders, gently lengthen the back of your neck (no aggressive “chin jam”).
-
Movement snacks: Every 30–60 minutes, stand up and do 5–10 slow shoulder rolls + 5 slow upper-back “open book” turns (pain-free range).
-
Sleep support: Try a pillow height that keeps your neck neutral (not cranked up or drooping).
-
Gentle shoulder blade squeeze: 2 sets of 8–12 reps, easy effort, keep neck relaxed.
If your pain is intense or highly irritable, a PT can help you find the right starting dose so you don’t flare it up.
What to avoid (at least for now)
These don’t “ruin” you—but they often keep symptoms stirred up early on:
-
Long periods looking down (phone/laptop) without breaks
-
Repeated end-range looking up/turning that reproduces arm symptoms
-
Heavy overhead lifting while pain is hot
-
Aggressive stretching that sends pain/tingling farther down the arm
-
“Pushing through” progressive numbness or weakness
When to seek urgent care
Get urgent medical evaluation if you have:
-
Progressive or significant arm/hand weakness (dropping things, can’t lift wrist/arm like usual)
-
Trouble with balance or walking, new clumsiness in hands, or widespread numbness (could suggest spinal cord involvement)
-
Loss of bowel/bladder control (rare with neck issues, but serious)
-
Fever/chills, unexplained weight loss, history of cancer, or constant night pain
-
Recent major trauma
-
Sudden severe headache, fainting, or new neurological symptoms (especially with neck pain)
Neck pain guidelines emphasize screening for serious pathology and referral when indicated.
When to see a physical therapist
Consider seeing a PT if:
-
Symptoms last more than 1–2 weeks without improvement
-
Pain is recurring or limiting work, sleep, or exercise
-
You have numbness/tingling that keeps returning
-
You’re unsure what movements are safe
-
You want a plan to rebuild strength and prevent flare-ups
In PT, you can expect a detailed assessment of neck motion, strength, sensation/reflexes, shoulder blade mechanics, and which positions help or irritate symptoms—then a progressive plan.
Within our clinic, people with neck-related nerve symptoms often also benefit from whole-spine and strength programming—especially if symptoms are influenced by posture and activity tolerance. You can see related service info here: Orthopedic & Sports Physical Therapy.
FAQ
Is pain inside the shoulder blade a sign of cervical radiculopathy?
It can be. Many people feel pain along the shoulder blade border or “inside” the shoulder blade with neck-related nerve irritation. It can also come from local muscle overload or upper-back joint irritation, which is why an exam matters.
Do I need an MRI right away?
Not always. Imaging is typically more helpful when there are red flags, progressive neurological changes, or symptoms that don’t improve with appropriate conservative care. Your clinician can guide that decision.
Will a chiropractor or PT adjustment fix it?
Some people feel short-term relief with manual techniques, but lasting improvement usually comes from pairing hands-on care with exercise and activity progression.
Should I stretch my neck a lot?
Gentle mobility can help, but aggressive stretching that increases arm symptoms is usually not the best move early on. A PT can show you the “just right” amount.
How long does it take to get better?
It varies. Many people improve over weeks with the right approach, but factors like symptom severity, irritability, and workload demands matter. If you’re not trending better—or weakness is worsening—get assessed.
Why Quincy Physical Therapy
At Quincy Physical Therapy, we take a spine-focused, strength-based approach: calm symptoms, restore motion, and build capacity so your neck and shoulder girdle can handle real-life demands. Care is individualized and progresses at a pace your nervous system can tolerate.
If you’d like help sorting out whether your shoulder blade and arm symptoms are coming from your neck—and what to do next—schedule an evaluation.
References
-
Blanpied PR, et al. Neck Pain: Revision 2017 Clinical Practice Guidelines. J Orthop Sports Phys Ther. 2017.
-
North American Spine Society (NASS). Diagnosis and Treatment of Cervical Radiculopathy from Degenerative Disorders. 2009 guideline (PDF).
-
Bier JD, et al. Physical Therapy Assessment and Treatment in Patients With Nonspecific Neck Pain (KNGF guideline; includes cervical radiculopathy). Phys Ther. 2018.
-
Fritz JM, et al. Exercise Only vs Exercise With Mechanical Traction for cervical radiculopathy. J Orthop Sports Phys Ther. 2014.
-
Xu X, et al. Manual therapy for cervical radiculopathy (systematic review). 2025.